CY 2024 Hospital Outpatient Prospective Payment System (OPPS) Final Rule
In November 2023, CMS published the CY 2024 Hospital Outpatient Prospective Payment System (OPPS) Final Rule that included required schemas for hospital machine-readable files (MRFs) as of 7/1/2024. CMS finalized this rule after an open comment period that resulted in feedback submissions from stakeholders all across the industry and patients as consumers.
As compared to the Proposed Rule, the Final Rule extends the grace period for the new required schemas, which will go into effect on 7/1/2024.
By 7/1/2024, hospitals and health systems must publish machine-readable files (MRFs) according to a standard format that includes new, more detailed data elements. CMS has coupled the required MRF format with additional measures designed to strengthen and automate enforcement efforts.
Implementation Timeline
In the public comment period that opened on the heels of the Proposed Rule, CMS received substantial feedback from hospitals needing more time to create new files that follow the required schema. As a result, the originally proposed 3/1/2024 deadline for implementing the standard template was extended a few months to 7/1.
While you might interpret some portions of the rule to indicate that a new deadline hasn’t been set, later verbiage confirms this to be true:
“…hospitals will be required to adopt a CMS template format beginning July 1, 2024.”
CMS also included Tables 151A and 151B to show clear implementation timelines of each respective requirement:
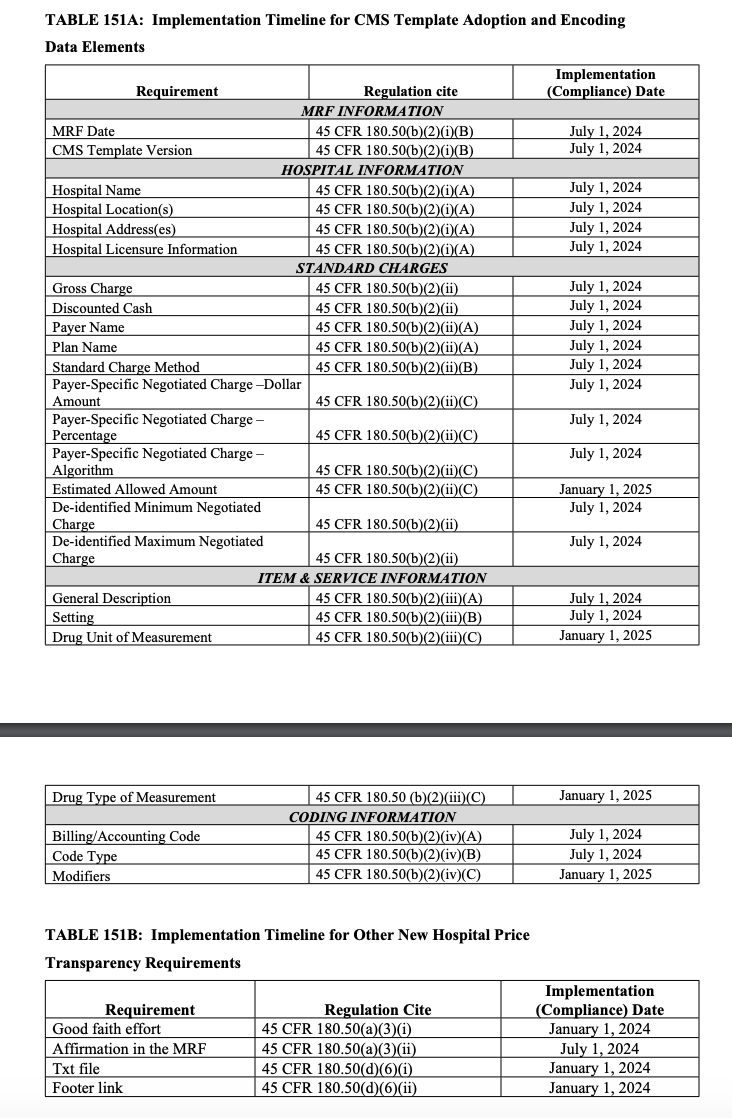
As documented above, usage of the template itself and most of the new data elements will be enforced on 7/1/24. However, there are some notable action items due on other dates as well:
As of 1/1/24, website display requirements go live. These include
- Placing a text file with a direct link to the MRF, and
- Placing a footer link to your price transparency information on the homepage of your hospital website
As of 1/1/25, some of the data elements that CMS acknowledges will take more time for providers to prepare, such as
- Estimated Allowed Amount (more details further in the blog), and
- Detailed drug information: drug unit of measurement and drug type of measurement
CMS Templates
Hospitals will need to choose between one of three allowed CMS MRF templates by 7/1. The templates are designed to be flexible enough to accommodate each hospital’s varying resourcing and display preferences: think the HGTV of schema formatting.
The JSON schema allows hospitals to efficiently display standard charge information in a clear, hierarchical manner with a relatively smaller file size. JSON files are commonly used in electronic data interchange and programming, and hospitals comfortable with this format can continue to use it moving forward.
In addition, CMS acknowledged that many hospitals may be more familiar with traditional CSV file formats or may not have all the technical resources for JSON file creation. For those hospitals, CMS created two templates:
CSV Wide: more columns, fewer rows
- additional columns added for each payer/plan combination to house the relevant payer-negotiated rate
CSV Tall: fewer columns, more rows
- column headers are static
- rows are added to house additional payer/plan combinations
According to the Final Rule, the majority of the MRFs that have been released thus far are typically most similar to the CSV Tall template. However, hospitals can choose whichever option reduces the operational burden of switching. CMS will also refresh the detailed instructions and data dictionaries for each on the newly-minted Github repository to incorporate updates from the Final Rule.
New Data Elements
Payer/Plan
Payer-negotiated rates must be associated with their respective payer and plan as two separate data elements. Providers who have not already separated these fields in their MRF should note that, when rates do not change between plans, the regulation allows for the creation of categories of plans based on the specific nature of their managed care agreements (e.g., “All PPO Plans”, “All Plans”). CMS is working to prevent files from becoming overly bulky due to repetitive rates across numerous plans.
Standard Charge Methodology (f/k/a Contracting Method)
Each payer-negotiated rate must now be accompanied by a description of the contract provision used to calculate the rate.
The current list of allowed values includes:
- case rate
- fee schedule
- percent of total billed charges
- per diem
- other
CMS suggested that including the methodology used will provide necessary context to the published rates while matching a similar Transparency in Coverage requirement of the Payer MRFs. Otherwise, users are unable to create an apples-to-apples comparison if they are inadvertently comparing a case rate to a per diem reimbursement methodology. This change should bolster the overall ecosystem of price transparency data by removing a lot of guesswork required to add meaning to dollar values that currently exist in hospital MRFs without a defined methodology.
Algorithmic Rates
In July’s OPPS Proposed Rule, CMS suggested a requirement that hospitals must specify when detailed algorithms (not the social media kind) are utilized to calculate a negotiated rate within the MRF. When a payer-negotiated rate cannot be listed as a dollar amount (for example, payment at a percent of total billed charges). The rationale in the Proposed Rule was focused on improving rates displayed in consumer-friendly tools. Ideally, patients would be able to receive a dollar value estimate based on the individual payer-specific negotiated charge.
While the Final Rule slightly walks back this requirement such that hospitals must only “describe” the algorithm rather than specify it, this will still require providers to elaborate on how each rate was calculated throughout the process of creating their MRFs. CMS committed to providing examples designed to help ensure providers are creating files that contain enough context about how the rate was calculated.
CMS Assessment and Enforcement
Several aspects of the new format are intended to drastically reduce CMS’ manual administrative effort required to locate and assess compliance with the Hospital Price Transparency Rule.
Effective 1/1/2024, hospitals will be required to add a footer link to their homepage directing users to price transparency resources. A footer link on the homepage adds a new level of standardization for gathering files. Furthermore, a text file must be added to the root folder of the site pointing to a download link of the current MRF, which CMS says they will soon provide more guidance on for non-technical staff. Essentially, CMS is doubling down on making MRFs easier to find, and alongside the requirements, they’re committed to providing a technical framework for hospital IT departments to utilize.
When we step back and absorb all these measures from the 10,000-foot view, we see a clear view of new MRF files and data elements that allow for more consistent and automated file review, assessment, and, where needed, enforcement actions by CMS.
Speaking of enforcement, another noteworthy change going into effect on 1/1/24 is that any compliance actions or assessments may now be publicized on the CMS website. Currently, CMS only posts a list of hospitals that received civil monetary penalties (CMPs). The Final Rule cited that nearly 1,000 warning notices had been issued to providers as of September 2023, while there are currently only 14 CMPs posted to the CMS website tracking enforcement actions.